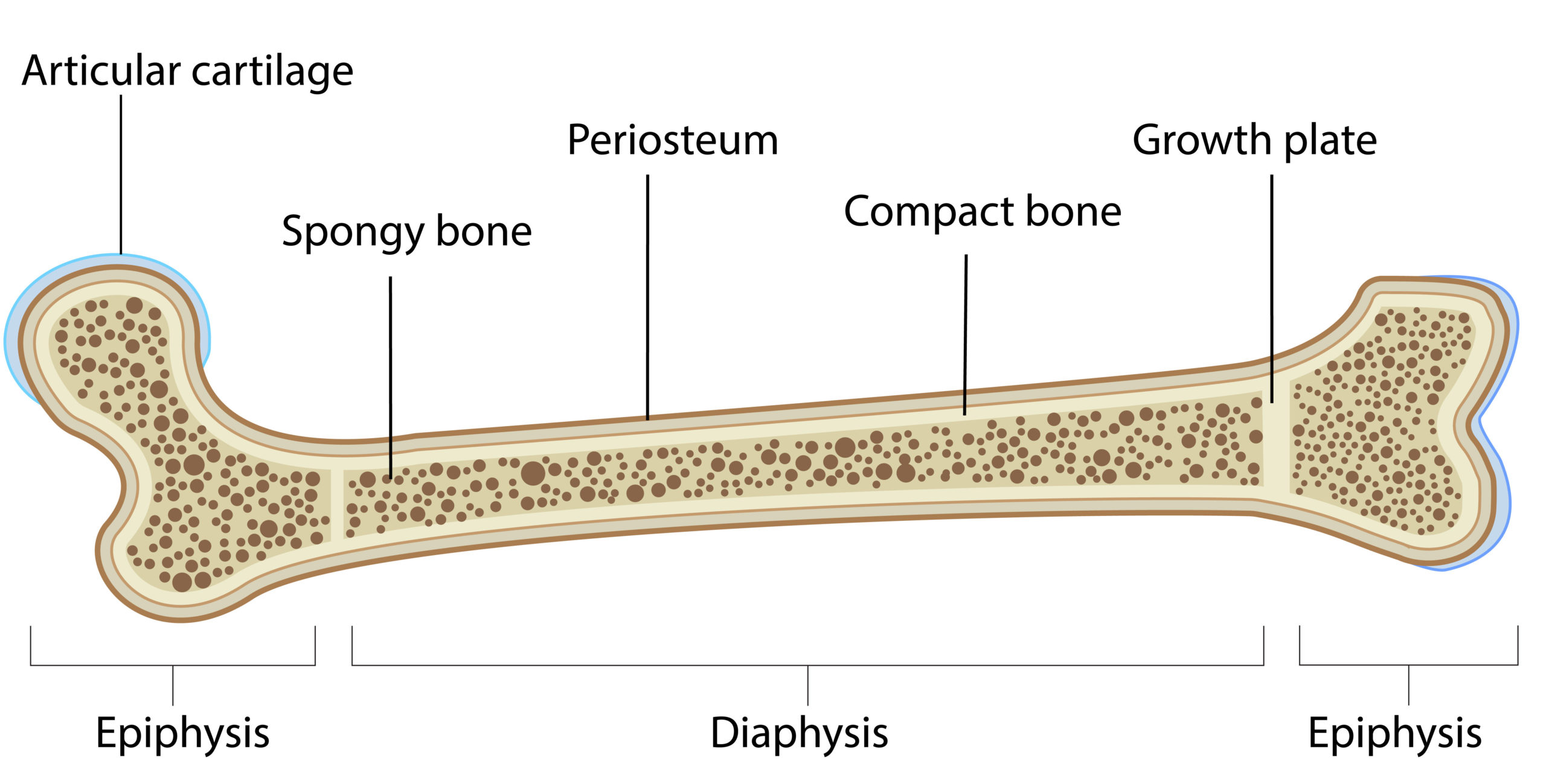
The growth plate is a special area on children’s bones that contains cells that allow the bone to get taller.
Growth plates are found on all long bones. The most commonly affected growth plates are those around the knee joint, the ankle joint, and the wrist joint.
From about 14 years to 16 years, the growth plate closes and so growth stops. Growth plate injuries are fairly common making up over 15% of childhood injuries.
Injuries to the growth plate can lead to early closure of the growth plate. This is medically called a growth arrest. This can be the whole growth plate or part of it. The blockage that develops in place of the growth plate is called a physeal bar.
In this article, we will discuss the different types of growth plate injuries, their sequelae, and treatment for growth plate injuries.

Do you need to see a paediatric orthopaedic surgeon?
Types of growth plate injuries
Growth plate fractures were initially classified by Salter and Harris and so in most medical literature, they are called Salter-Harris fractures.
This fracture classification describes where the fracture enters and exits the bone. There are 5 types of growth plate injuries.
- Salter harris type 1
The fracture line goes through the growth plate itself without breaking into the bone near it. On the x-ray, it may appear like the growth plate has slipped out of place.
- Salter-Harris type 2
In salter Harris type 2 fractures, the fracture line goes through the growth plate and exits out through the metaphysis.
- Salter-Harris type 3
In salter Harris type 3 fractures, the fracture line goes through the growth plate and exits out through the epiphysis. The epiphysis is what makes up the joint surface in children.
- Salter-Harris type 4
In salter Harris type 4 fractures, the fracture line goes through the growth plate and exits out through both the metaphysis and the epiphysis.
- Salter-Harris type 5
Type 5 fractures are often diagnosed in retrospect when the child later presents with growth arrest. These ones result from a loading impact that crushes the growth plate.
Treatment of growth plate injuries
Just like any fracture, growth plates are fractures that need to be stabilized in order to heal. Most growth plate fractures are healed in 6 to 8 weeks depending on the age of the child.
Non-operative treatment
Just like most fractures in children, growth plate fractures can be treated non-surgically if there is very little or no displacement of the fracture.
In this case, they are treated in a cast.
Operative treatment
Surgical treatment of growth plate injuries is reserved for:
- Fractures displaced more than 2mm especially those extending to the joint surface.
- Fractures that require more stabilization beyond a cast.
Operative treatment involves holding the bones with pins or screws and sometimes small plates.
Sequelae of growth plate fractures
Growth plate injuries can lead to growth closure. Morphologically, the growth plate is made of cartilage, and when it closes off, that area changes to bone.
The closed-off area on the growth plate is called a bony bar or physeal bar. The growth plate can either close off fully or partially.
- Full growth plate closure. When the whole growth plate closes off, the bone ceases to grow any longer. This can be seen in form of limb length discrepancy where one leg or arm is shorter than the other.
- Partial growth plate closure. In partial growth arrest, part or side of the physis stops growing while the other continues. This leads to development of an angulated deformity. This may lead to bowed knees or arms etcetera.
Treatment of growth arrest
The treatment depends on the kind of growth plate injury present and the age of the child.
- Physeal bar excision. This is a kind of surgery that involves cutting away the physeal bar. This is done if the physeal bar is less than 30% of the total growth plate.
- Angular deformity correction. This depends on the severity and location of the deformity. There are many surgical techniques that can be used for the correction of these deformities. This can be done through guided growth techniques or osteotomies.
In conclusion, growth plate injuries are categorized into 5 types and can be treated either non-surgically or operatively. the complication associated with these injuries is growth plate closure.